Erfolgreich durch internationale Zusammenarbeit
Morphology, Pathology, Physiology
Cite as: Archiv EuroMedica. 2022. 12; 4: e1. DOI 10.35630/2199-885X/2022/12/4.6
SPECIFIC
FEATURES OF X-RAY ANATOMY AND PROFILOMETRY IN PEOPLE WITH DIFFERENT
TYPES OF FACIAL SKELETON
Sergey
Dmitrienko1 ,
Taisiya Kochkonyan2 ,
,
Taisiya Kochkonyan2 ,
Vladimir Shkarin1 ,
Dmitry Domenyuk3,5  ,
,
Tatiana Dmitrienko1 ,
Stanislav Domenyuk4
1 Volgograd
State
Medical University, Volgograd;
2 Kuban
State Medical University, Krasnodar;
3 Stavropol
State Medical University, Stavropol;
4 North
Caucasus Federal University, Stavropol;
5Pyatigorsk
Medical and Pharmaceutical Institute − Branch of the Volgograd
State Medical University, Pyatigorsk, Russia
 download article (pdf)
download article (pdf)
domenyukda@mail.ru
Abstract
This
work is a summary of results obtained through clinical, radiological,
and photometric studies involving 90 people (aged 18-25) with
physiological types of bite. The first stage of the study implied an
assessment of the face main anatomical structures location (chin,
lips and jaws) relative to the conventionally accepted and proposed
lines (planes) of the teleroentgenogram and face profile images. At
the second stage, the patients were divided into three groups
featuring different types of dental arches – mesotrusive (n=33),
protrusive (n=30) and retrusive (n=27), depending on the incisor
angle of the antagonizing medial incisors. Almost all patients of
Group 1 were observed to have the upper lip touching the nasal line
passing through the n (nasion) and the sn (subnasale) points, the
lower lip receding backwards and the occlusal relationships falling
within the age norm, while the average incisor angle being
135.24±3.09°. In most patients of Group 2, the upper and lower lips
were located forward from the nasal line, while the occlusal
relationships matched the age norm, and the average incisor angle was
116.24±3.02°. In Group 3, the patients’ upper and lower lips were
located behind the nasal line, the occlusal relationships
corresponding to the age norm and the average incisor angle making up
146.24 ± 3.34°. The obtained data expand the vision of the upper
and lower lip facial topography for various dental arches, and are of
applied importance when it comes to assessing the aesthetic profile
of soft facial tissues, as well as the data in question can serve the
criteria to evaluate the rehabilitation effectiveness in patients
with dental pathology in view of their individual maxillofacial
features.
Keywords:
profilometry, X-ray anatomy, face soft-tissue profile, facial
aesthetics, facial skull, physiological occlusion, dental arch,
mesotrusion, retrusion, protrusion.
INTRODUCTION
Thorough
investigation into the normal variability of the human cranial
morphology, as well as the structure and patterns of its development,
are of reasonable research and pragmatic interest for clinical
experts involved in dentistry (surgical, orthopedic, general),
orthodontics, maxillofacial surgery, neurosurgery, and ophthalmology
[9,16,20,24,31,37,49,66].
The
applied value of orthodontics, which is a complex diverse discipline,
implies not only correcting issues affecting the position of teeth,
the dental arch shape (size), and the bite, yet also in ensuring the
correct growth of the jaws, improving the shape of the facial skull,
bringing back to normal the dental function, restoring facial
aesthetics, guiding the development of adjacent body organs and
systems as a whole [1,12,19,26,40,55,61].
Orthodontic
treatment, which includes arriving at morphological, functional and
aesthetic optimum through any age stage, is to be implemented
employing both conventional methods that have long proven effective
in correcting dental issues and deformities at the early stages of
their development, and advanced innovative technologies and treatment
techniques that allow taking therapeutic and preventive measures in
case of obvious anomalies and deformities of the dental apparatus
[2,21,29,33,47,51,67].
Dental
anomalies and deformations mainly come accompanied by significant
morphological, functional and aesthetic issues. There are significant
changes in the facial features to be observed as well as distortion
affecting the proportions of the face and its parts, which leads to a
serious deterioration in facial aesthetics, at the same time working
a negative effect on the patient’s psycho-emotional and social
status [4,13,35,48,54,60,64].
Clinical
studies have revealed a reliable effect that orthodontic treatment
has on the face soft tissues position. The face soft-tissue profile
contour is under a significant influence of the teeth movement
degree, of the mandibular joint articular head position, of the
pressure that soft tissues have on the dentition, of the adjustment
capacity of the dentition system ligament set, as well as other
factors [3,8,41,46,57,62].
The
issues related to identifying the right proportion determining the
harmonious maxillofacial structure are rated among the key tasks in
terms of orthodontic diagnostics and treatment planning [7,58].
Constitutionally
significant facial features, taken as objects for thorough study
within aesthetic dentistry, include: the gnathic face type (meso-,
dolicho-, brachygnathic); the head facial part growth (neutral,
horizontal, vertical); masticatory muscles thickness and spatial
orientation; the mandible morphological (angle) and morphometric
features (condyle width, angular width) [6,22,27,36,43,44,50,56].
There
is scientific evidence showing that morphological and the
craniofacial anatomical features, which are based on skeletal, dental
and soft tissue indicators, should rely not on race and ethnicity
alone, yet also on factors like age and sex variability, if we talk
about normal structure vs. various dental pathologies [45]. The study
of the face soft-tissue profile is of value when it comes to a more
complete representation of the patient’s individual features, the
specifics and harmony of the face, the proportion of the face parts,
the face profile convexity or concavity degree, as well as in terms
of planning the orthodontic treatment tactics to eliminate anomalies
related to the dental system evolution [5,30,59].
Experts
have offered convincing proof revealing that the position of the
front teeth, i.e. protrusion or retrusion, can have an effect on the
lips position, even in case of physiological occlusal relationships
[10,18,23,28,38].
The
currently employed classifications of dental arches use terms
defining the arcade (gnathic) type while taking into account index
values and dental indicators based on the teeth size or the dental
arch length [11,15,17,32,42,53,65].
Systematizing
scientific data can help conclude that orthodontic treatment should
aim at maintaining facial parameters or contribute to their
improvement, while orthodontic correction, if carried out to improve
aesthetics and help achieve occlusive and facial balance, points at
the modern approach to planning complex dental treatment [14,25,52].
Shaping
an understanding of the face soft-tissue parameters and their
variability within the physiological norm allows designing a
treatment plan aimed both at eliminating dental issues as well as at
harmonizing the face of each individual. Despite numerous items
published in this field, the issue of determining the interdependence
between the frontal teeth trusive position and the lips aesthetic
position has not been covered to sufficient extent, which explains
the reason behind this study.
Aim
of study. To carry out a comparative analysis of various methods to be used for
identifying the location of the facial main anatomical structures and
to detect the specific features for the lips location in people
revealing different trusive types of dental arches with physiological
occlusion of permanent teeth.
MATERIALS
AND METHODS
The
study involved young people aged 18-25, with respective written
consent obtained and approved by the local Ethics Committee. Stage 1
of the study involved matching the location of the face main
anatomical structures (chin, lips and jaws) in view of the generally
accepted and proposed lines (planes) as reflected in the
teleroentgenogram and in the face profile photographs (Fig. 1).
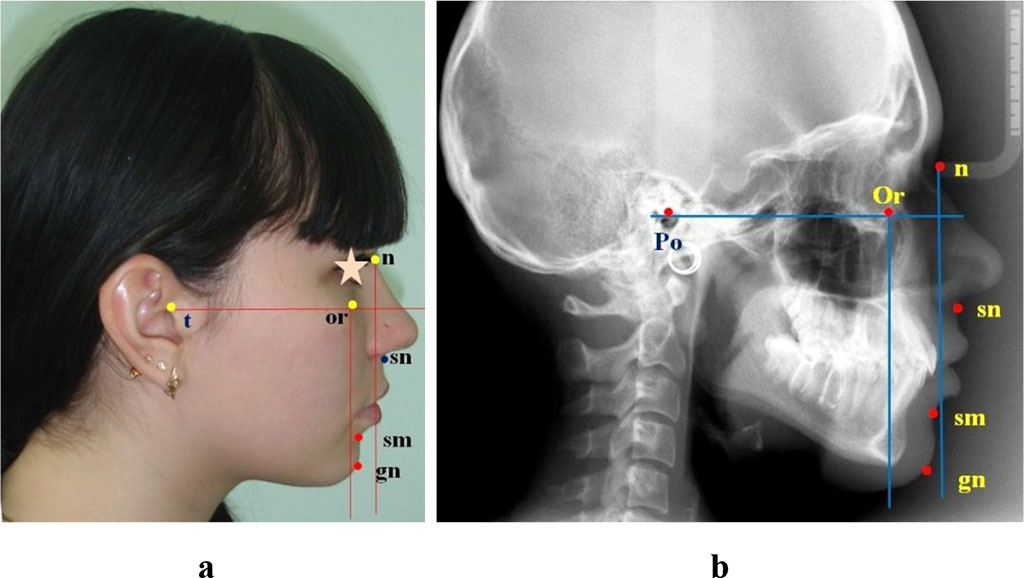
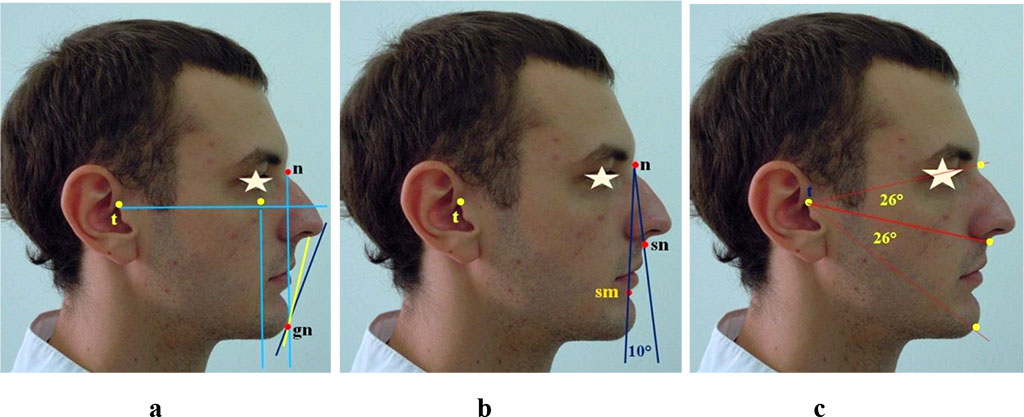
Figure
1 – comparative analysis of the main anatomical structures location
in relation to the lines, photo (a), teleroentgenogram (b)
There
was the Frankfort horizontal drawn, with a nasal and an orbital
vertical designed perpendicular to it subject to the guidelines as
accepted conventionally in orthodontics.
The
profile images were used to analyze the lips position in relation to
Rickett’s line, which ran connecting the nose tip with the chin,
and Steiner’s line, which connected the chin and the nasal septum
ventral restriction (the middle between the nose tip and the subnasal
point). Besides, the upper lip and the lower jaw position was
identified along the lines shaped by the nasal-subnasal and
nasal-supramental verticals while measuring the profile angle between
these mark points (Fig. 2).
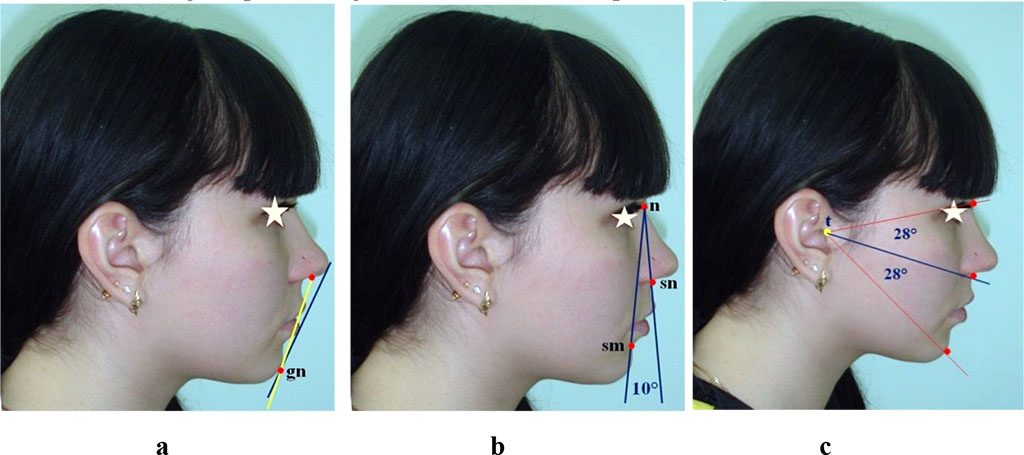
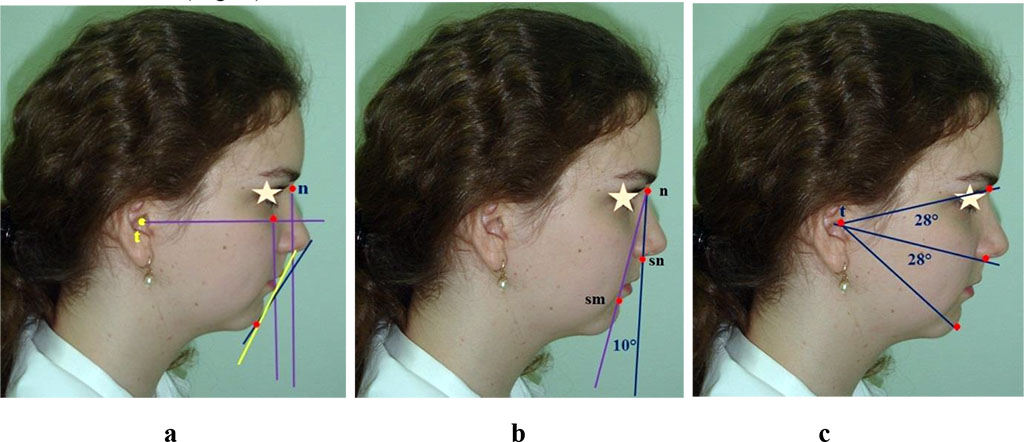
Figure
2 – comparative analysis of the anatomical structures location in
relation to Rickett’s and Steiner’s aesthetic facial lines (a),
nasal verticals (b) and radial facial lines (c)
The
radial lines running from the tragion (t) point to the sn,
sm points were used to identify the proportional balance of the nasal
and gnathic parts of the face.
Stage
2 of the study involved 90 patients, and in view of the antagonizing
medial incisor angle, which reveals the trusive type of dental
arches, the patients were divided into three groups – Group 1
(n=33) were patients with the mesotrusive type of dental arches
(inter-incisal angle – 125°-140°); Group 2 (n=30) included
patients with the protrusive type of dental arches (inter-incisal
angle – below 125°), and Group 3 (n=27) were patients with the
retrusive type of dental arches (inter-incisal angle – above 140°)
(Fig. 3). All the patients had an optimal incisor overlap, both
vertical and horizontal.
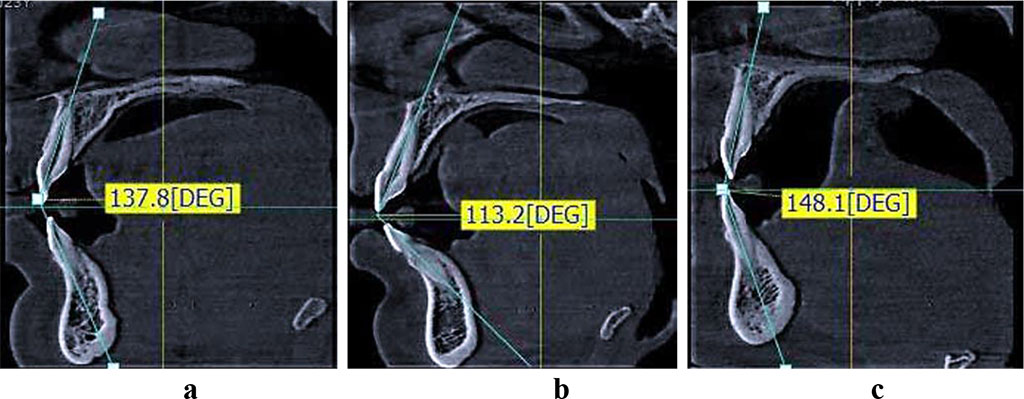
Figure
3 – types of medial incisors location on the CBCT: a – patients
of Group 1 (mesotrusive dental arches); b – patients of Group 2
(protrusive dental arches); c - patients of Group 3 (retrusive dental
arches).
Also,
the trusion of dental arches was identified in view of the gnathic
(arcade) and dental indicators to be found in modern classifications.
The mesotrusive type was observed in people with meso-arcade
normodontia, dolicho-arcade microdontia and brachy-arcade macrodontia
dental arches. The protrusive type included dental arches falling
within the dolicho-arcade (macro- and normodentia) and meso-arcade
macrodontia types. The anterior teeth retrusion was observed in
people with brachy-arcade arches with their micro- and normodontia,
as well as with meso-arcade microdontia type dental arches
[34,39,63].
RESULTS
AND DISCUSSION
People
with physiological occlusion and mesogenic face type were observed to
have the location of the lips, if taken in relation to Rickett’s
and Steiner’s lines, close to normal; the upper lip, though,
typically failed to reach Rickett’s line and was somewhat protruded
in relation to Steiner’s line (Fig. 4).
Figure
4 – Specific features of the anatomical structures location in
relation to Rickett’s and Steiner’s aesthetic lines (a), nasal
verticals (b) and radial lines (c) in case of the mesogenic face type
When
analyzing the position of the upper lip in relation to the initial
line, it was noted that the upper lip more often touched the
specified landmark. The profile angle, which determines the position
of the jaws, and which is shaped by the nasal and the
nasal-supramental vertical lines was within the normal range –
about 10 degrees. The radial lines separating the nasal and gnathic
parts of the face matched the normal values constituting an average
of 28.43+0.62
degrees.
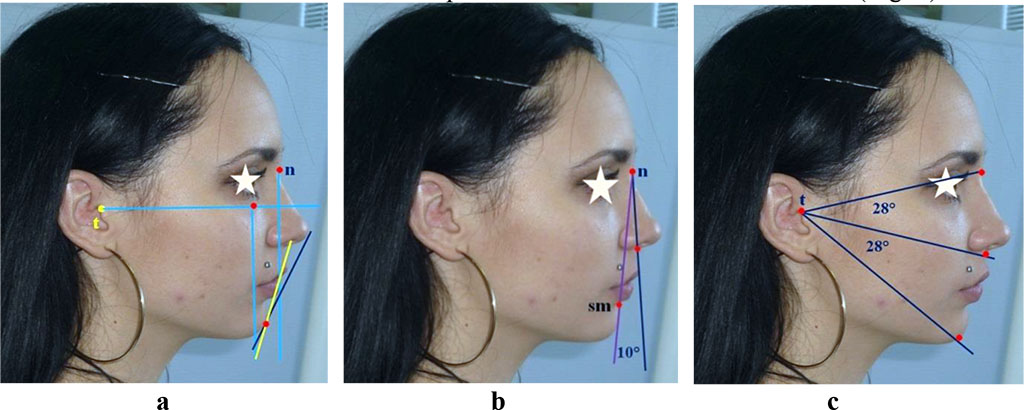
It
was noted that people with physiological occlusion and the progenic
face type had their lips not reaching Rickett’s and Steiner’s
lines, which can be explained by the chin extended forward and
reaching Dreyfus’s nasal vertical (Fig. 5).
Figure
5 – Specifics of the anatomical structures location in relation to
Rickett’s and Steiner’s face aesthetic lines (a), nasal verticals
(b) and radial lines (c) in case of the progenic face type
An
analysis of the upper lip position in relation to the nasal line
revealed that the upper lip, as a rule, touched the specified mark.
The profile angle, which determines the jaws relative position and
makes up the nasal and the nasal-supramental vertical lines fell
within the normal range being about 10 degrees. The radial lines
separating the nasal and the gnathic parts of the face matched the
normal values making up an average of 27.12+0.94
degrees. People with physiological occlusion and the retrogenic face
type featured the lips reaching Rickett’s and Steiner’s lines,
which could be accounted for by the chin location behind Simon’s
orbital vertical (Fig. 6).
Figure
6 – Specific features of the anatomical structures location in
relation to Rickett’s and Steiner’s face aesthetic lines (a),
nasal verticals (b) and radial lines (c) in case of the retrogenic
type of face
When
analyzing the upper lip position in relation to the nasal line, the
upper lip, as a rule, it was noted to be touching the mark in
question. The profile angle, which determines the relative position
of the jaws and is shaped by the nasal and the nasal-supramental
vertical lines was within the normal range at about 10 degrees. The
radial lines separating the nasal and the gnathic parts of the face
matched the norm with an average of 28.17± 0.56 degrees.
Through
Stage 2 of the study, we identified the lips position taking into
account the trusive type of dental arches (Fig. 7)
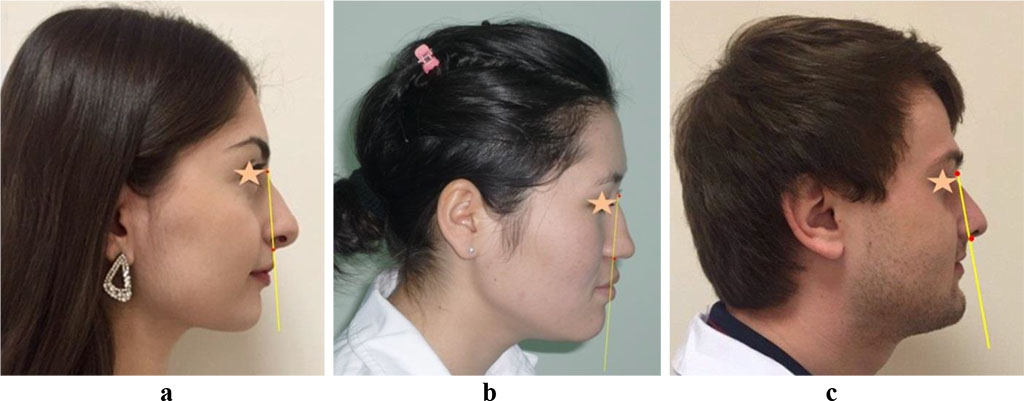
Figure
7 – The lips position in case of mesotrusive (a), protrusive (b)
and retrusive types of dental arches (c)
The mesotrusive
type of dental arches more often came along with various types of the
meso-arcade normodontia type, with 24 patients featuring this, which,
if expressed in relative numbers, was 26.67+0.49%
of the total number of patients. Dolicho-arcade microdontia arches
were observed in patients (6.67±0.28%), whereas brachy-arcade
macrodontia dental arches were found in 3 patients (3.33±0.2%).
Virtually all the patients of this group had the upper lip touching
the nasal line, the lower lip showing somewhat posterior retreat, the
occlusal relationships matching the age norm, and the inter-incisal
angle being 135.24 ± 3.09 degrees. In 30 patients (33.33±0.52%)
with the protrusive
type of dental arches, meso-arcade macrodontia types were more common –
in 15 persons, i.e., 16.67± 0.41% of the total number of the
patients. Dolicho-arcade normodontia arches were identified in 9
patients (10.0±0.33%), whereas dolicho-arcade macrodontia arches
were to be seen in 6 patients (6.67±0.28%). Almost all the patients
of this group had the upper and lower lips in an anterior position
from the nasal, while the occlusal relationships fell within the age
norm, the inter-incisal angle being 116.24 =3.02 degrees. As far as the
retrusive type of dental arches is concerned, more common were here the
brachy-arcade microdontia types – in 15 patients, that accounting
for 16.67 ± 0.41% of the total number of the patients. Brachy-arcade
normodontia arches were identified in 8 patients (8.89=0.32%), and
meso-arcade microdontia dental arches in 4 patients (4.44=0.23%).
Almost all patients of this group had the upper and lower lips
located behind the nasal line, while the occlusal relationships
matched the age norm, and the inter-incisal angle was 146.24+3.34
degrees.
The
above means that the method proposed for identifying the lips
position based on the nasal line can be employed to evaluate their
location aesthetics in view of the individual morphological features
pertaining to the facial gnathic part.
CONCLUSIONS
- Based
on the regularities identified in the facial skull structure, the
detected correlation between the morphometric parameters of the
dental arches, jaws, facial bone structures, as well as the
relationship between the facial and cerebral skull bones and the
soft-tissue profile contour, a method was proposed for evaluating
the lips facial contour position in people with physiological
occlusion and various trusive types of the dental arches.
- When
constructing a nasal line on a profile photostatic image, the first
anthropometric mark relies on the upper nasal n (nasion) point, the other anthropometric mark point being the
profile subnasal sn (subnasale) point.
- The
upper lip was observed to touch the nasal line mainly in people with
the mesotrusive type of dental arches and physiological occlusal
relationships. In patients with protrusive type of dental arches and
physiological occlusion, the upper and lower lips were mostly in an
anterior position relative the nasal line, while in case of
physiological retrusion of the frontal teeth, the upper and lower
lips were typically located behind the nasal line.
- The
newly obtained data offered above will expand and complement the
ideas to be found in respective research literature focusing the
topography of the upper and lower lips facial contour in patients
with different types of dental arches, and are of great importance
in terms of data verification when evaluating the aesthetic profile
of the face soft tissues, while taking into account individual
features, as well as the results of aesthetic and morphofunctional
rehabilitation of patients suffering from dental pathologies.
REFERENCES
- Ackerman
J.L., Proffit W.R.
Soft tissue limitations in orthodontics: Treatment planning
guidelines. The
Angle Orthod.
1997;67(5):327-36.
DOI: 10.1043/0003-3219(1997)067<0327:STLIOT>2.3.CO;2.
- Arnett
G. W., Bergman R.T.
Facial keys to orthodontic diagnosis and treatment planning. Part I.
American
journal of orthodontics and dentofacial orthopedics. 1993. −
Vol.103, pt. l. − P. 299-312. DOI: 10.1016/0889-5406(93)70010-L.
- Arnett
G. W., Bergman R.T.
Facial keys to orthodontic diagnosis and treatment planning. Part
II. American
journal of orthodontics and dentofacial orthopedics. 1993. −
Vol.103, pt. 2. − P. 395–411. DOI: 10.1016/0889-5406(93)70010-L.
- Avanisyan
V., Al-Harazi G. Morphology
of facial skeleton in children with undifferentiated connective
tissue dysplasia. Archiv
EuroMedica.
2020. Vol. 10; 3: 130-141. https://dx.doi.org/10.35630/2199-885X/2020/10/3.32
- Becker
I. M. Comprehensive Occlusal Concepts in Clinical Practice / I. M. Becker.
– John Wiley & Sons, 2010. – 316 p.
- Bennett
J. C., McLaughlin R. P. Orthodontic management of the dentition with the preadjusted
appliance. – Isis Medical Media, 1997. – 380 р.
- Bisharа,
S.E. Textbook of Orthodontics. Mosby. – 2001. − 592 р.
- Borodinа V.V. Biometry of permanent occlusion dental arches – comparison
algorithm for real and design indicators. Archiv
EuroMedica.
2018. Vol. 8. № 1.
P. 25-26.
DOI: 10.35630/2199-885X/2018/8/1/25
- Brand
R.W., Isselhard D.E. Anatomy of Oral structures. 7th ed. Mosby co. St. Louis; 2003.
- Carlson,
James E. Physiologic occlusion [Text] / James E. Carlson. – UK: – St
Louis: Mosby, 2009. –218 р.
- Davydov
B.N. Algorithm for determining the size of artificial teeth by the
morphometric parameters of the face in people with full adentia. Dentistry.
2018; 97(6): 57-60.
DOI – 10.17116/stomat20189706157
- Davydov
B.N., Budaychiev G.M-A. Changes of the morphological state of tissue of the paradontal
complex in the dynamics of orthodontic transfer of teeth
(experimental study). Periodontology,
2018; Vol. 23; 1-23(86): 69-78. DOI:10.25636/PMP.1.2018.1.15
- Davydov,
B.N. Improving diagnostics of periodontal diseases in children with
connective tissue dysplasia based on X-ray morphometric and
densitometric data. Periodontology.2020;25(4):266-275.
(in Russ.) https://doi.org/10.33925/1683-3759-2020-25-4-266-275.
- Dawson
P.E. Functional
Occlusion: From TMJ to Smile Design / P. E. Dawson. – Elsevier
Health Sciences, 2006. – 647 p.
- Diggs,
D. B.: The
quantification of arch form. Ph.D. thesis, University of Washington,
1962.
- Dmitrienko
S.V. Enhancement of research method for spatial location of
temporomandibular elements and maxillary and mandibular medial
incisors. Archiv
EuroMedica.
2019. Vol. 9. № 1. P. 38-44. https://doi.org/10.35630/2199-885X/2019/9/1/38
- Dmitrienko
S.V. Modern classification of dental arches. Archiv
EuroMedica.
2014.
Vol.
4.
№ 2. P. 14-16.
- Dmitrienko
T.D. Connection between clinical and radiological torque of medial
incisor at physiological occlusion. Archiv
EuroMedica.
2019. Vol. 9. № 1. P. 29-37. https://doi.org/10.35630/2199-885X/2019/9/1/29
- Domenyuk
D.A. Algorithm for forecasting the shape and size of dent arches front
part in case of their deformations and anomalies. Archiv
EuroMedica. 2017.
Vol.7.
№ 2. Р.
105-110.
- Domenyuk
D. A. Anatomical and topographical features of temporomandibular joints in
various types of mandibular arches. Medical
News of North Caucasus.
2019;14(2):363-367. DOI –
http://dx.doi.org/10.14300/mnnc.2019.14089 (In Russ.)
- Domenyuk
D.A., Kochkonyan T.S., Shkarin V.V.
Conceptual
approach to diagnosing and treating dentoalveolar transversal
divergent occlusion. Archiv
EuroMedica.
2022. 12; 3: e1. DOI 10.35630/2022/12/3.25
- Domenyuk
D.A., Kochkonyan T.S. Implementation of neuromuscular dentistry principles in
rehabilitation of patients with complete adentia. Archiv
EuroMedica. 2022.
Vol. 12; 2: 108-117. https://doi.org/10.35630/2199-885X/2022/12/2.29
- Domenyuk
D.A. Major
telerenthengogram indicators in people with various growth types of
facial area. Archiv
EuroMedica.
2018. Vol.
8; 1: 19-24. https://doi.org/10.35630/2199-885X/2018/8/1/19
- Domenyuk
D. Structural
arrangement of the temporomandibular joint in view of the
constitutional anatomy. Archiv
EuroMedica.
2020. Vol.
10. № 1. Р.
126-136. https://doi.org/10.35630/2199-885X/2020/10/37
- End
E. Physiological Occlusion of Human Dentism: Diagnosis & Treatment
/ E. End. – Verlag Neuer Merkur GmbH, 2006. – 192 p.
- Fischev
S.B., Puzdyryova M.N. Morphological
features of dentofacial area in peoples with dental arch issues
combined with occlusion anomalies. Archiv EuroMedica. 2019. Vol. 9;
1: 162-163. https://doi.org/10.35630/2199-885X/2019/9/1/162
- Fomin
I.V. Effect of jaw growth type on dentofacial angle in analyzing lateral
teleradiographic images. Archiv
EuroMedica.
2019. Vol. 9; 1: 136-137. https://doi.org/10.35630/2199-885X/2019/9/2/136
- Ghamdan
Al.H. A
method for modeling artificial dentures in patients with adentia
based on individual sizes of alveolar arches and constitution type. Archiv
EuroMedica.
2021. Vol. 11; 1: 109–115. https://doi.org/10.35630/2199-885X/2021/11/1.25
- Ghamdan
Al.H. Occlusal
plane orientation in patients with dentofacial anomalies based on
morphometric cranio-facial measurements. Archiv
EuroMedica.
2021. Vol. 11; 1: 116–121. https://doi.org/10.35630/2199-885X/2021/11/1.26
- Graber
L. W., Vanarsdall R. L., Vig K. W. L., Huang G. J. Orthodontics:
Current Principles and Techniques. – Elsevier, 2016. – 928 p.
- Grinin
V.M., Khalfin R.A. Specific features of grinder teeth rotation at physiological
occlusion of various gnathic dental arches. Archiv
EuroMedica.
2019. Vol. 9; 2: 168-173. https://doi.org/10.35630/2199-885X/2019/9/2/168
- Grinin
V.M., Khalfin R.A. Specific features of transversal and vertical parameters in lower
molars crowns at various dental types of arches. Archiv
EuroMedica.
2019. Vol. 9; 2: 174-181. https://doi.org/10.35630/2199-885X/2019/9/2/174
- Harutyunyan
Yu. Undifferentiated connective tissue dysplasia as a key factor in
pathogenesis of maxillofacial disorders in children and adolescents. Archiv
EuroMedica.
2020. Vol. 10; 2: 83-94. https://dx.doi.org/10.35630/2199-885X/2020/10/2.24
- Ivanyuta
O.P., Al-Harasi G. Modification
of the dental arch shape using graphic reproduction method and its
clinical effectiveness in patients with occlusion anomalies // Archiv
EuroMedica.
2020. Vol. 10; 4: 181-190. https://dx.doi.org/10.35630/2199-885X/2020/10/4.42
- Ivanov
S.Yu., Lepilin A.V. Morphological specifics of craniofacial complex in people with
varioustypes of facial skeleton growth in case of transversal
occlusion anomalie. Archiv
EuroMedica.
2019. Vol. 9; 2: 5-16. https://doi.org/10.35630/2199-885X/2019/9/2/5
- Kochkonyan
T.S., Al-Harazi G. Clinical types of hard palatal vault in people with various gnathic
dental arches within physiologically optimal norm. Archiv
EuroMedica.
2022. Vol. 12; 1: 91-98. https://dx.doi.org/10.35630/2199-885X/2022/12/1.20
- Kochkonyan
T.S., Al-Harazi G. Specific features of variant anatomy and morphometric
characteristics of the palatal vault in adults with different
gnathic and dental types of arches. Archiv
EuroMedica.
2021. Vol. 11; 3: 54-60. https://dx.doi.org/10.35630/2199-885X/2021/11/3/14
- Kochkonyan
T. S., Shkarin V. V. Study of the profile of the soft tissues of the face, taking into
account the individual typological features of the dental arches. Medical
Alphabet.
2022;(7):99–108. https://doi.org/10.33667/2078-5631-2022-7-99-108
- Kochkonyan
T.S., Al-Harazi G. Morphometric patterns of maxillary apical base variability in people
with various dental arches at physiological. Archiv
EuroMedica.
2021. Vol. 11; 4: 123-129. https://dx.doi.org/10.35630/2199-885X/2021/11/4.29
- Kochkonyan
T.S., Shkarin V.V., Dmitrienko
S.V.
Morphological
features of dental arch shape and size within baby teeth bite
period. Archiv
EuroMedica.
2022. 12; 3: e1. DOI 10.35630/2022/12/3.23
- Kochkonyan
T.S., Shkarin V.V. Variant anatomy of transitional occlusion dental arch at optimal
occlusal relationships. Archiv
EuroMedica.
2022. Vol. 12; 2: 128-133. https://dx.doi.org/10.35630/2199-885X/2022/12/2.32
- Kondratyeva
T. Methodological approaches to dental arch morphology studying. Archiv
EuroMedica.
2020. Vol. 10; 2: 95-100. https://dx.doi.org/10.35630/2199-885X/2020/10/2.25
- Korobkeev
A. A. Anatomical and topographical features of temporomandibular joints in
various types of mandibular arches. Medical
News of North Caucasus.
2019;14(2):363-367. DOI –
http://dx.doi.org/10.14300/mnnc.2019.14089 (In Russ.).
- Korobkeev А.A. Anatomical features of the interdependence of the basic parameters
of the dental arches of the upper and lower jaws of man. Medical
news of North Caucasus.
2018. – Vol. 13. – № 1-1. – P. 66-69. (In Russ., English
abstract). DOI – https://doi.org/10.14300/mnnc.2018.13019
- Korobkeev
A. A. Variability of odontometric indices in the aspect of sexual
dimorphism. Medical
News of North Caucasus.
2019;14(1.1):103-107. DOI –
https://doi.org/10.14300/mnnc.2019.14062 (In Russ.).
- Lepilin
A.V. A
biometric approach to diagnosis and management of morphological
changes in the dental structure.
Archiv EuroMedica. 2020. Vol. 10; 3: 118-126. https://dx.doi.org/10.35630/2199-885X/2020/10/3.30
- Lepilin
А.V., Puzdyrova M.N., Subbotin R.S. Dependence of stress strain of dental hard tissues and periodontal
on horizontal deformation degree. Archiv
EuroMedica.
2019. Vol. 9; 1: 173-174. https://doi.org/10.35630/2199-885X/2019/9/1/173
- Lepilin
А.V., Fomin I.V., Budaychiev G.M. Improving
odontometric diagnostics at jaw stone model examination. Archiv EuroMedica.
2018. Vol. 8; 1: 34-35. https://doi.org/10.35630/2199-885X/2018/8/1/34
- Mazharov
V. N. Peculiarities of the orientation of the occlusion plane in people
with different types of the gnathic part of the face. Medical
News of North Caucasus.
2021;16(1):42-46. DOI – https://doi.org/10.14300/mnnc.2021.16011
(In Russ.)
- McNamara
J.A. Orthodontic and Dentofacial Orthopedics. Needfarm Press. Inc., 1998.
555 p.
- McLaughlin
R. P., Bennett J. C., Trevisi H. J. Systemized orthodontic treatment mechanics. – Elsevier Health
Sciences, 2001. – 324 р.
- Nanda
R. Esthetics and biomechanics in orthodontics [Text] / R. Nanda. –
Oxford University Press in the UK: CRC Press.– 2015 – 612 р.
– ISBN: 978-1-4557-5085-6
- Porfiriadis
M.P. Classification
of facial types in view of gnathology. Archiv euromedica,
2017. Vol. 7. № 1. P. 8-13.
- Porfiriadis
M.P., Budaychiev G.M-A. Dentoalveolar specifics in children with cleft palate during
primary occlusion period. Archiv
EuroMedica.
2018. Vol. 8; 1: 33-34. https://doi.org/10.35630/2199-885X/2018/8/1/33
- Porfiriadis
M.P. mathematic
simulation for upper dental arch in primary teeth occlusion. Archiv euromedica,
2018. Vol. 8. № 1. P. 36-37. https://doi.org/10.35630/2199-885X/2018/8/1/36
- Porfiriadis
M.P. Setting
reference points for key teeth location in case of abnormal dental
arch shape. Archiv euromedica,
2017. Vol. 7. № 2. P. 111-117.
- Proffit
R.W. Contemporary Orthodontics / R.W. Proffit // 6rd ed. St Louis, Mo:
Mosby, 2018. – 744 p.
- Rufenacht
C. R. Principles
of esthetic integration. – Chicago: Quintessence Pub. Co, 2000. –
248 p.
- Slavicek,
R. The Masticatory Organ: Functions and Dysfunctions / R. Slavicek. –
Klosterneuburg: Gamma Med. Fortbildung, 2002. – 544 p.
- Suetenkov
D.E., Firsova I.V., Kubaev A. A
modified method for rapid palatal expansion anchored on
mini-implants. Archiv
EuroMedica.
2022. Vol. 12; 1: 84-90. https://dx.doi.org/10.35630/2199-885X/2022/12/1.19
- Shkarin
V.V., Grinin V.M., Khalfin R.A.
Specific features of central point location between incisors in
people with physiological occlusions // Archiv
EuroMedica.
2019. Vol. 9; 2: 165-167. https://doi.org/10.35630/2199-885X/2019/9/2/165
- Tefova
K., Dmitrienko T., Kondratyeva T. Modern
x-ray diagnostics potential in studying morphological features of
the temporal bone mandibular fossa. Archiv
EuroMedica.
2020. Vol.
10. № 1. Р.
118-127. https://doi.org/10.35630/2199-885X/2020/10/36
- Vedeshina
E G., Dmitrienko S.V. Correlation of dental arch major linear parameters and odontometric
indices given physiological occlusion of permanent teeth in various
face types. Archiv
EuroMedica.
2016. Vol. 6; 2: 18-22.
- Vedeshina
E G. Efficiency
evaluation for integrated approach to choice of orthodontic and
prosthetic treatments in patients with reduced gnathic region. Archiv
EuroMedica.
2015. Vol. 5; 2: 6-12.
- Vedeshina
E G., Dmitrienko S.V. Mistakes in Pont (Linder-Hart) method used for diagnosing abnormal
dental arches in transversal plane. Archiv
EuroMedica.
2016. Vol. 6; 2: 23-26.
- Weisheim
L.D., Melekhow S.V. Analytical approach within cephalometric studies assessment in
people with various somatotypes. Archiv
EuroMedica.
2019. Vol. 9; 3: 103-111. https://doi.org/10.35630/2199-885X/2019/9/3.29
- Zelensky
V.A., Anfinogenova O.I., Pushkin S.V. Peculiarities of phosphorine calcium exchange in the pathogenesis of
dental caries in children with diabetes of the first type. Entomology and Applied Science Letters. 2018.
Vol.5.
№ 4. Р.
49-64.
back
